
Blood supply to heart involves coronary circulation, the functional blood supply to the heart muscle itself. Collateral routes play role in blood delivery to heart even if major vessels are occluded.
Coronary circulation: Arterial supply
Two coronary arteries take part in supplying of the blood and arise at the root of the aorta. These arteries include,
Left coronary artery (LCA)- Left anterior descending (LAD)/ interventricular artery. It is a marginal artery. LCA is basically circumflex artery.
Right coronary artery (RCA)- Marginal artery. RCA is known as Posterior inteventricular artery. Atial and nodal arteries, LCA supplies blood to the apical parts of heart, and 2/3rd of interventricular septum via LAD. Circumflex ranch- supplies the lateral and post.
RCA Supplies
Right coronary artery blood supplies involves,
- Right ventricle
- Interventricular septum (posterior 1/3rd part).
- Inferior part of left ventricle.
- Conducting system except left ranch of bundle of his supplied by LCA.
Heart Sound Due To (Lub-Dub) Due To Valves Closing
- ‘’Lub’’-closing of atrioventricular valve
- “Dub’’-closing of semilunar valves
Arterial Blood supply to heart
Right and left coronary arteries provide arterial supply of the heart which arises from the ascending aorta immediately above the aortic valve.
The right coronary gives posterior interventricular artery and supply conduction system, such hearts are right dominance. In 10% cases posterior interventricular artery come from circumflex artery which supply posterior interventricular septum as well as AV node, such hearts are left dominance.
Venous drainage and lymphatics
Venous drainage is through the variable coronary veins and the coronary sinus. The lymphatic vessels mainly drain into:
- Brachiocephalic nodes, in front of the bracheiocephalic veins
- Tracheobronchial nodes, present at the distal end of the trachea
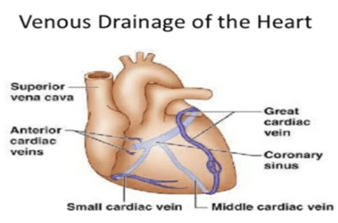
Most blood from the wall of heart drains to the right atrium with the help of the coronary sinus, which is present in the posterior part of the atrioventricular groove. It is a continuation of the great cardiac vein and opens into the right atrium to the left to the inferior vena cava.
Nerve blood supply to the heart
Sympathetic and parasympathetic fibers of the autonomic nervous system innervate the heart via the cardiac plexuses situated below the arch of the aorta. The main control and function of the heart lies with the medulla oblangata.
There is a part called the cardioacceleratory centre, or pressor centre, in the upper part of the medulla oblongata and an area called the cardioinhibitory centre, or depressor centre, located in the lower part. Together, they are known as the cardioregulatory centre, as they interact to control heart rate.
Sympathetic and Parasympathetic
The nervous supply to the heart is an autonomic processing which consists of both sympathetic and parasympathetic nervous system.
Sympathetic: The sympathetic fibers arise from the pressor centre, while the parasympathetic fibers arise in the depressor centre. The sympathetic nervous system functions on the sinoatrial node, accelerating the depolarisation rate, and therefore increasing the heart rate.
Parasympathetic– The parasympathetic system works in reverse in order to slow the heart rate down. The heart itself consists of a natural pacemaker, the sinotarial node, which does not require a nervous supply to function properly. If you sever all the nerves to the heart, then it will beat faster than normal, since there is normally a parasympathetic supply slowing the hear down.
Heart conduction system
Heart conduction system includes self-excitable specialized cardiac muscle fibers. They repeatedly generate action potentials that trigger heart contractions and act as pacemaker, and form conduction system. Heart conduction system consists of SA, AV node, and bundle of purkinje fibers.
An electrical conduction system administers the pumping of the heart and time duration of the contraction of various chambers. Heart muscle contracts in response to the electrical stimulus received system generates electrical impulses and conducts the throughout the muscle of the heart, stimulating the heart to contract and pump blood.
SA node, actually, acts as natural pacemaker. It is faster than other auto rhythmic fibers initiating 100 times per second. Nerve impulses from autonomic nervous system (ANS) and hormones regulate timing and strength of the each heartbeat.
Beginning in sinoatrial (SA) node in right atrial wall, blood propagates through atrial via gape junctions. Atrias contract and blood eaches atrioventricular (AV) node in inter septum entering atrioventricular bundle. Only site where action potentials are conducted manipulate from atria to ventricles due to fibrous skeleton. Blood then enters right and left bundle branches which extend through interventricular septum toward apex. Finally, large diameter fibers conduct action potential to remainder of ventricular myocardium.
Venous return of heart
Most of the venous blood supply return to heart occurs through the coronary sinus. Venae cardis minimi/ thebesian vein and anterior cardiac veins directerly drain into the right atrium.
Blood flow to heart during systole and diastole
During systole movement when heart muscles contract, it compresses the coronary arteries that is why blood flow is less. Flow of blood to the subendocardial surface of the left ventricle during systole is not there, so, this area is vulnerable to the ischemic damage and most common site of myocardial infarction.
Coronary blood flow
During systole, coronary blood flow to the right side is not much affected. This is because pressure difference between the aorta and right ventricle is much greater during systole than during diastole. Therefore more blood flows to the right ventricle during systole movement. Coronary blood flow in human beings at rest condition is about 225-250 ml/minute, about 5% of the cardiac output.
At rest, the heart extracts 60-70% of oxygen from each unit of blood delivered to heart ( other tissue extract only 25% of O2.
Factors affecting blood flow to coronary arteries
Following factors affect the rate of blood flow to coronary arteries:
- Pressure in aorta
- Chemical factors
- Neural factors
Note that coronary blood flow shows considerable autoregulation.
Innervations of heart
Innervations of heart may include parasympathetic vagus and recurrent laryngeal. Both form superficial and deep cardiac plexus, sympathetic upper 4 to 5 thoracic segment of spinal cord. The superficial plexus lies in the concavity of the aortic arch, and a deep plexus between the aortic arch and the trachea.
Both connect closely to each other. The deep cardiac plexus is formed by the cardiac nerves derived from the cervical ganglia of the sympathetic trunk. Also there are the cardiac ranches of the vagus and recurrent laryngeal nerves other than the superior cardiac branch of the left aympathatic trunk and the lower superior cervical cardiac branch of the left vagus nerve which form superficial plexus.
Superficial plexus is formed by the superior cardiac ranch of the left sympathetic trunk and the lower superior cervical cardiac ranch of the left vagus nerve. Their branches are the deep part of the plexus, to the anterior coronary plexus; and to the left anterior pulmonary plexus.
Anatomical basis of referred pain from heart
The pain sensation is carried by the middle and inferior cervical cardiac branches and thoracic cardiac ranches of sympathetic chain to thoracic ganglion of sympathetic chain. From here, impulses passes via the white rami of thoracic spinal nerve.
The central process of the neuron in dorsal root ganglion carries impulses to posterior horn of T-1 to T-5 spinal segment mainly or left side.
Also read: Cardiovascular Diseases: Leading Cause of Deaths Globally

















